From Call to Case/Chart: Standardizing Intake Data Capture and CRM/EHR Handoffs for High-Volume Inbound Teams
By Rick AlovisLast modified: September 1, 2026
Voted Top Call Center for 2024 by Forbes
Virtual Receptionists
Save time and money with our virtual receptionists.
AI Receptionist
AI-powered receptionist that answers, routes, and qualifies calls 24/7.
Enterprise Solutions
Solutions designed to scale with your organization’s needs.
Legal Services
Our virtual legal receptionists are experts in legal intake.
Last modified: September 1, 2026
High-volume inbound teams live or die by the last 120 seconds of the interaction: what gets captured, how it gets coded, and whether the handoff to your CRM, case management system, or EHR is clean enough to run without rework.
This guide is for enterprise and multi-location service organizations, intake-heavy legal teams, and healthcare practices that need consistent outcomes across overflow, after-hours coverage, and distributed staff. You will learn how to standardize intake data capture, design call disposition (wrap-up) codes, map fields across systems, and build reliable handoffs that protect quality and compliance.
Treat every call, chat, or web lead as a controlled pipeline with five stages: Capture, Normalize, Validate, Route, and Handoff. The goal is conversation to structured data with minimal interpretation.
When volume climbs, intake becomes a throughput problem. Teams start optimizing for speed, and data becomes close enough until downstream users (case managers, schedulers, billers, attorneys, clinicians) spend hours fixing it.
The root cause is usually not training effort. It is a lack of standard definitions and a lack of enforcement at the moment of capture.
Define the small set of fields required before a record can be handed off: identity, context, routing keys, source, and consent. Small enough for peak traffic, strict enough to prevent rework.
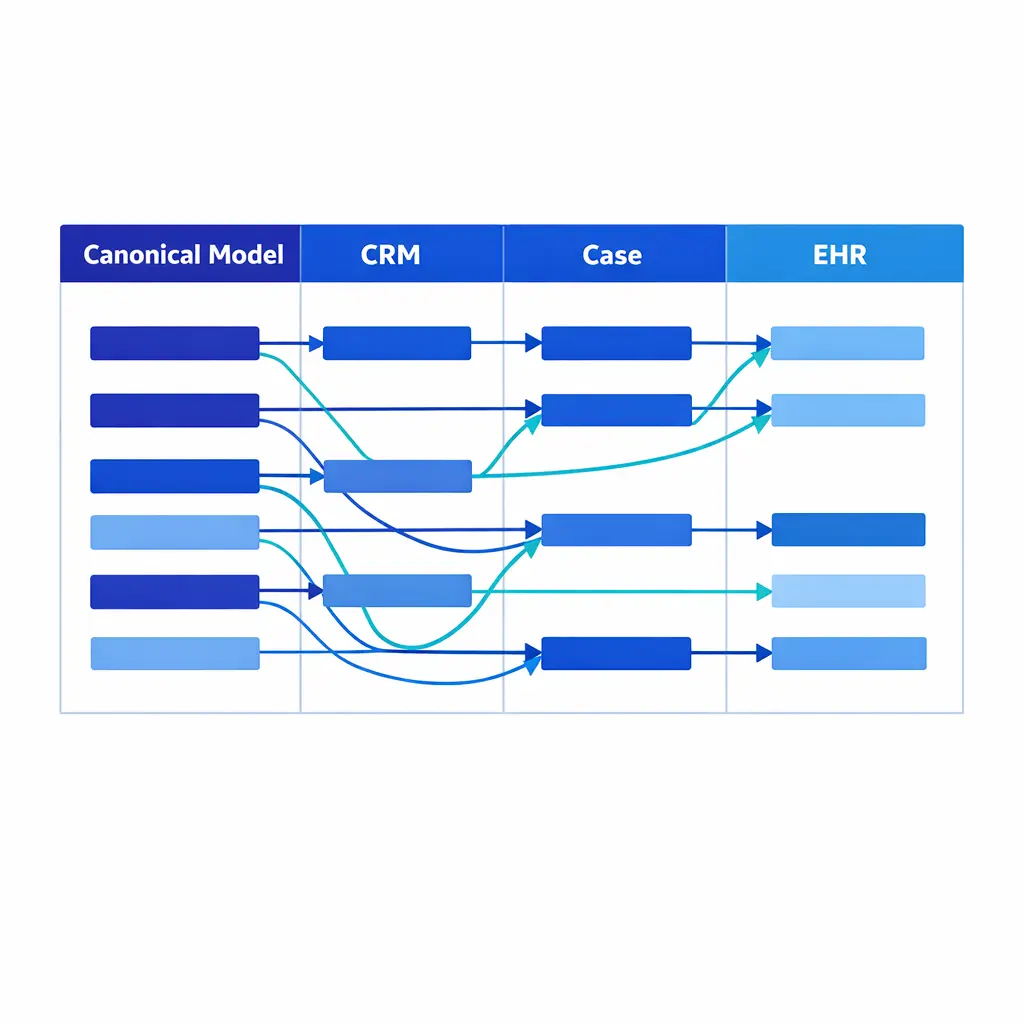
Start from a canonical intake model, then map it into each destination. That reduces vendor lock-in and stops every integration from inventing its own meaning of the data.
A dependable intake operation treats every call, chat, or web lead as the start of a controlled pipeline. Your goal is to move from conversation to structured data with minimal interpretation.
Standardize the pipeline in five stages so you can scale staffing without scaling error rates.
Use a structured intake form as the primary artifact. Free-text notes are valuable, but they should enrich the record, not define it.
Design your form so agents can complete the case/chart viable minimum in under two minutes, then optionally collect expansion fields when the call allows.
Disposition (wrap-up) codes classify the outcome and the next required action. Keep them simple enough to use and specific enough to drive routing, staffing, and pipeline reporting.
Normalization is where teams win back hours. Every field should have a single definition, a single format, and an approved list of values when applicable.
Examples: use one phone format, one best callback time format, one source taxonomy, and a consistent location identifier.
Check phone, email, required demographics, location, and new-vs-existing identity at capture, so downstream teams never discover a missing date of birth or invalid ZIP.
Validation is the difference between a record that exists and a record that works. Validate the basics at the edge: phone, email, required demographics, jurisdiction/location, and is this new vs existing identity resolution.
Do not rely on downstream teams to discover that a date of birth is missing, a ZIP code is invalid, or a caller's name is in the wrong field.
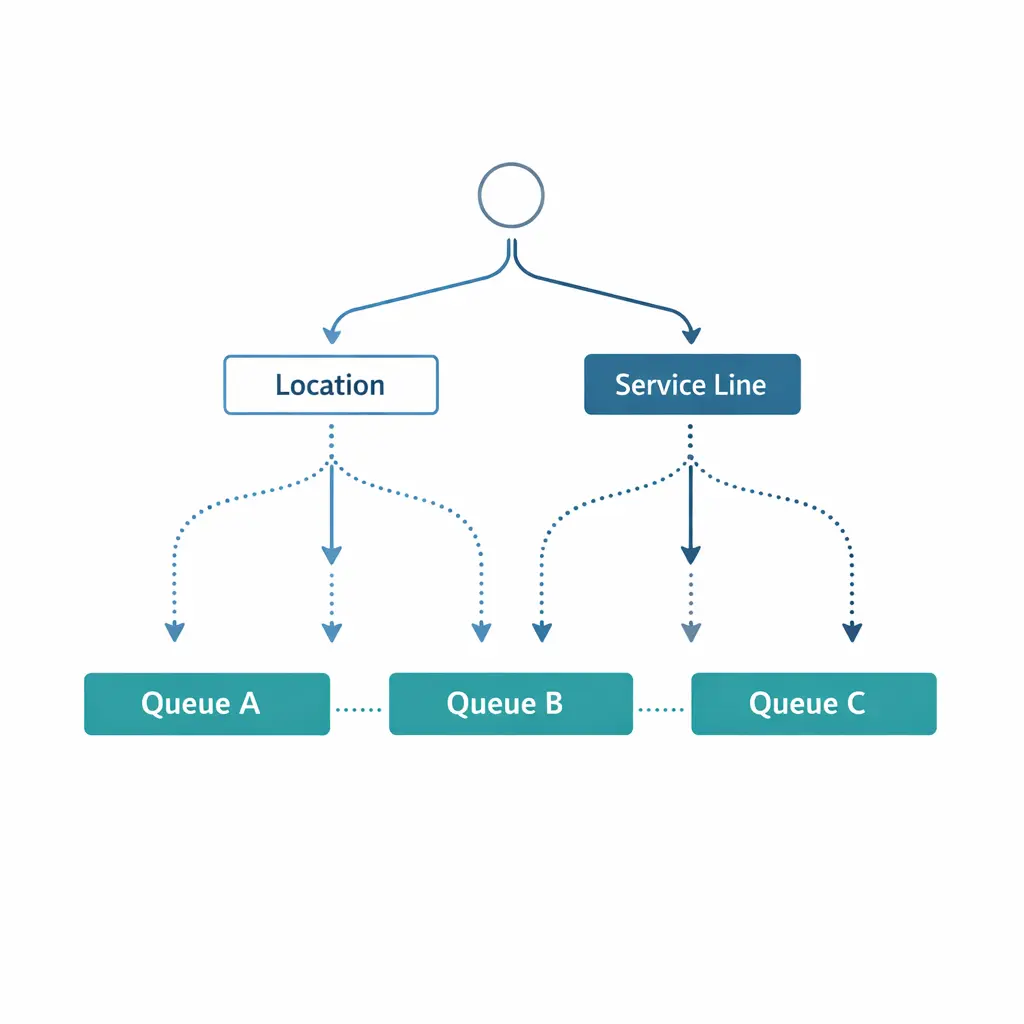
Drive routing from structured fields and dispositions, not agent memory. Deterministic routing lets overflow and after-hours coverage run without creating mystery work the next day.
Routing rules should be driven by structured fields and dispositions, not by the agent's memory of what to do. If two intake specialists handle different practice areas, or two clinics handle different payor networks, routing should be deterministic.
When routing is consistent, you can safely run overflow and after-hours coverage without creating mystery work the next day.
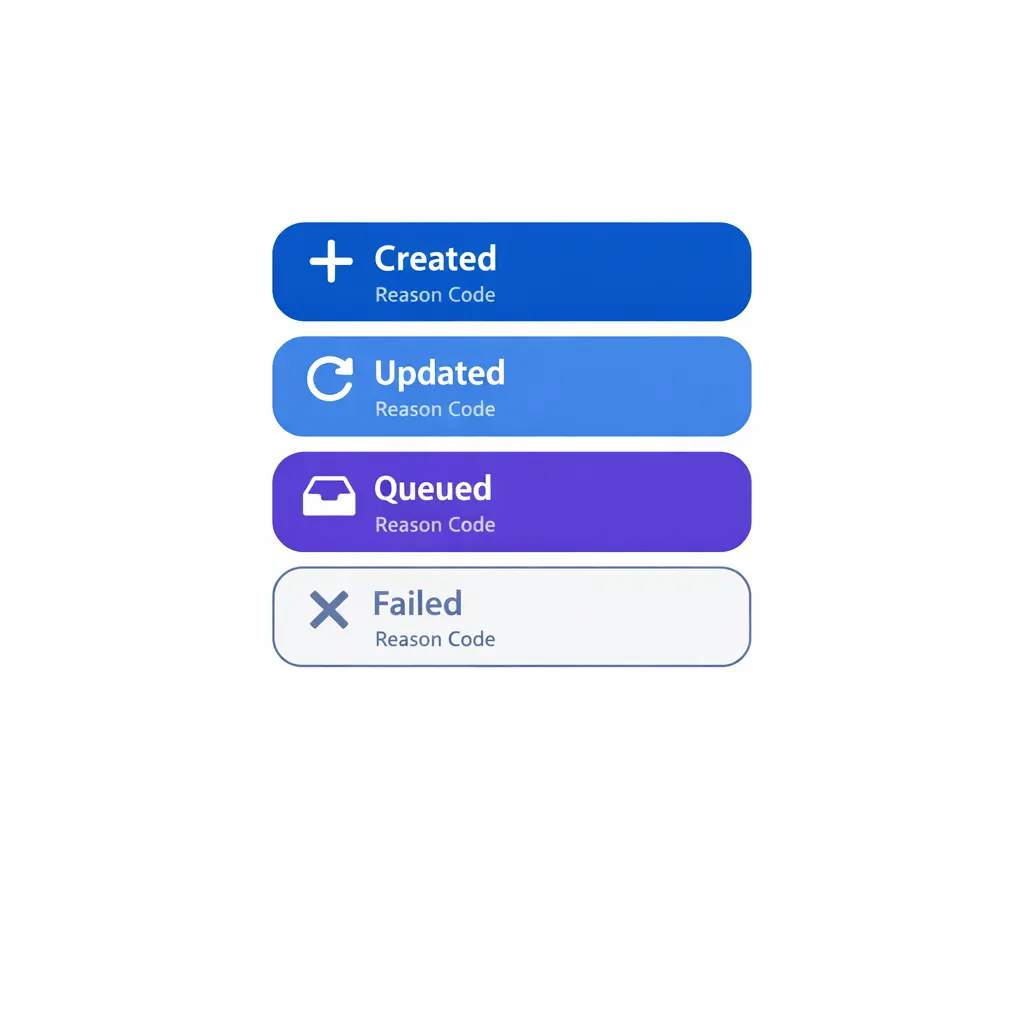
A handoff is complete only when the destination system confirms created, updated, or queued for review, with status visible to agents and supervisors so failures are fixed the same day.
A handoff is not complete when the agent clicks submit. It is complete when the destination system confirms one of three outcomes: created, updated, or queued for review due to a specific exception.
Build handoffs that return a visible status to agents and supervisors so failures are handled the same day, not discovered in weekly reporting.
When a match is uncertain, a critical field is missing, or an exception fires (payer not found, conflict check required), route the record to a clear queue-for-review lane.
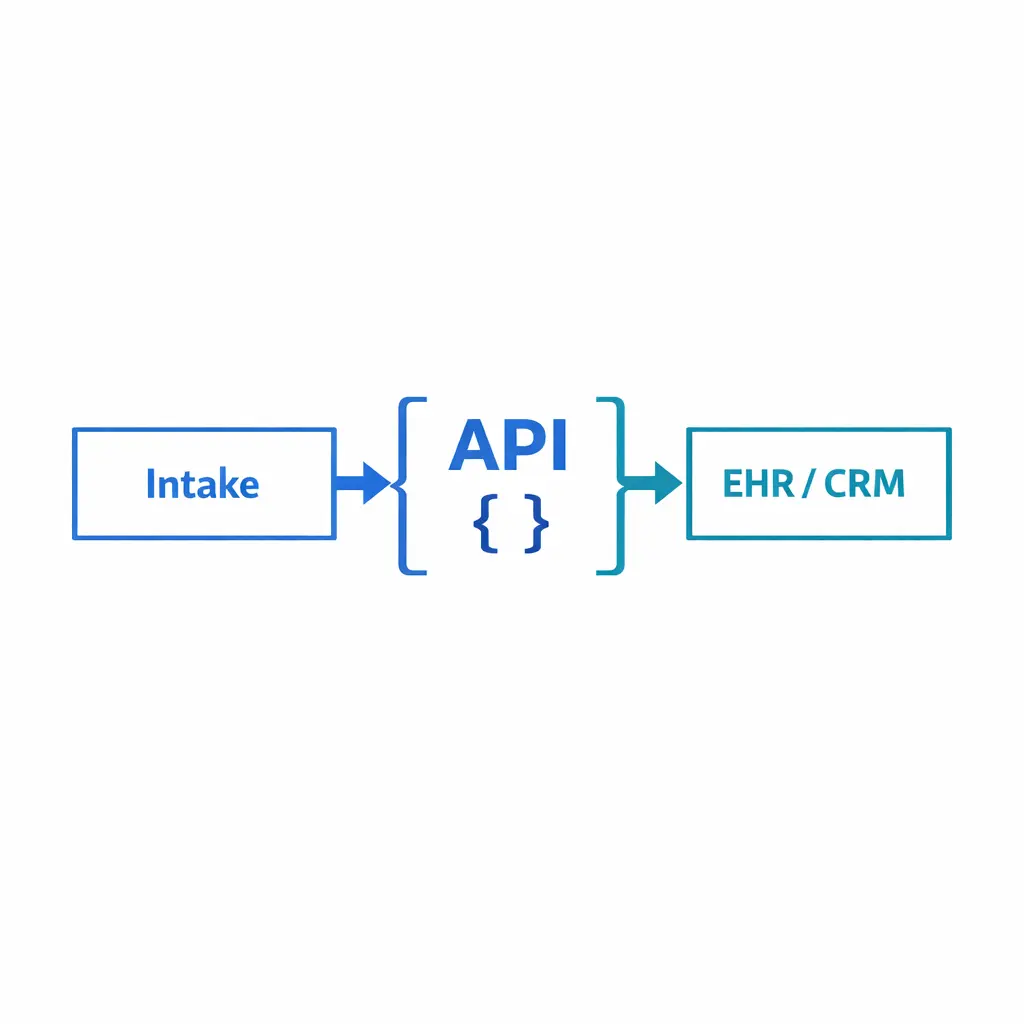
Start with a canonical intake model: a stable set of fields that represent what the business needs, independent of any single tool. Then map that canonical model into each destination system.
This reduces vendor lock-in and prevents each integration from inventing its own interpretation of what the data means.
Define a minimum dataset that must be captured before a record can be handed off. Keep it small enough to be realistic during peak traffic, but strict enough to prevent downstream rework.
A consistent source taxonomy turns intake into reportable ROI. Avoid defaulting to other; apply the same source values everywhere.
Expansion fields improve conversion and preparedness, but they should not block creation. Use conditional logic (if possible) so agents only see what matters for the scenario.
Free-text drift breaks reporting and routing. Approved value lists and structured fields keep the same concept from being typed ten different ways.
Disposition codes (also called wrap-up codes) are the operational language that turns conversations into measurable work. When standardized, they power routing, staffing decisions, coaching, and accurate pipeline reporting.
The goal is not to describe everything that happened on the call. The goal is to classify the outcome and the next required action.
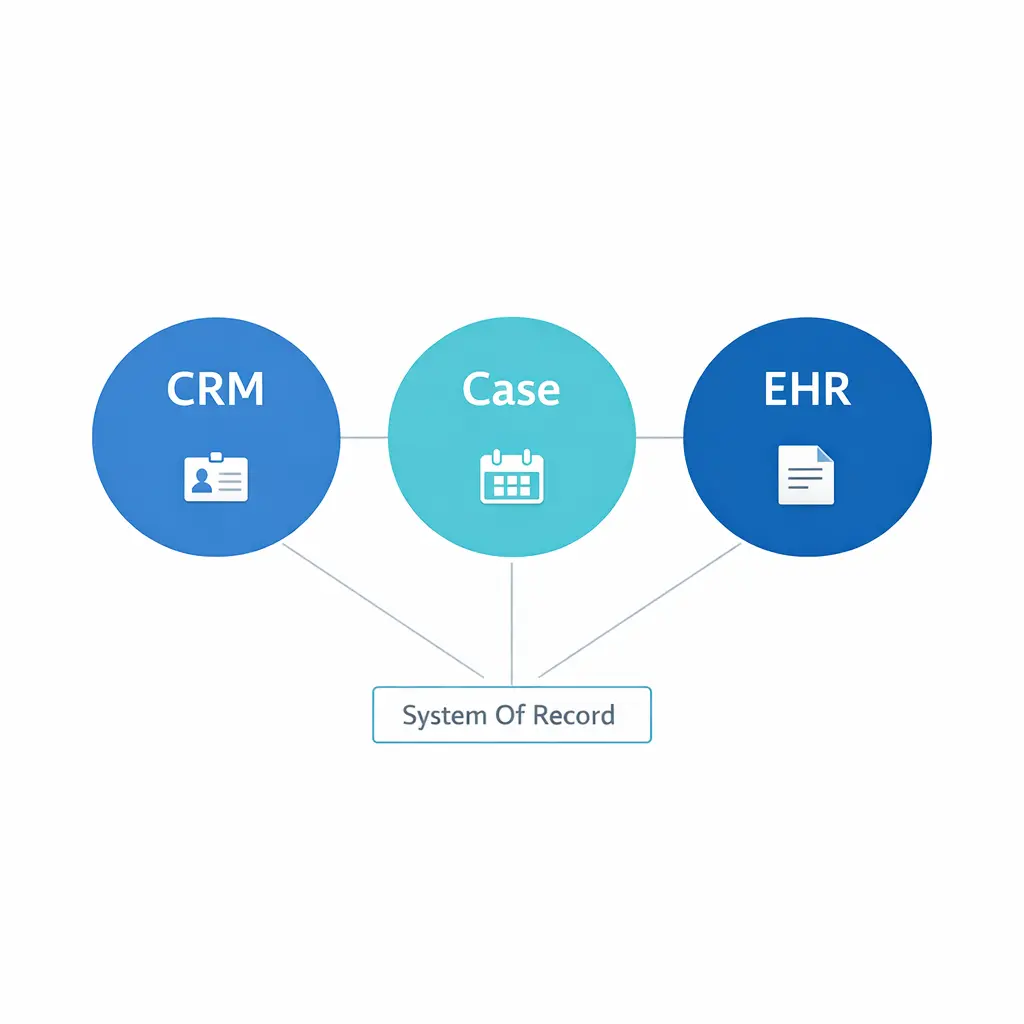
Decide which system owns each field. If the EHR owns demographics, the CRM should not become a competing copy without a deliberate plan.
Disposition chaos usually happens when different leaders add codes to answer one-off questions. The fix is governance: a clear owner, a change process, and a quarterly review tied to reporting needs.
Keep a published disposition dictionary that includes: definition, when to use, when not to use, required fields, and the downstream system action.
Match-confidence scoring decides new vs existing records, so updates land on the right case or chart instead of creating duplicates.
Field mapping is where most integration projects quietly fail. Teams map what is easy, not what is necessary, and then wonder why staff still retype data.
Use a mapping approach that separates data capture from system-specific storage, so your operation can evolve without rebuilding the world.
Even if you cannot book during the call, capture visit intent, constraints, and coverage cues so scheduling afterward is fast and accurate.
Most organizations need more than one handoff pattern because not every record can be fully automated. The trick is to make each pattern explicit and measurable.
Expansion fields improve conversion but should never block creation. Conditional logic shows agents only what matters for the scenario.
In healthcare, scheduling is often the highest-value outcome of intake. Even when you cannot fully schedule during the call, you can standardize what gets captured so scheduling is fast and accurate afterward.
When integrations are possible, interoperability approaches frequently center on standards like HL7 FHIR (Fast Healthcare Interoperability Resources), which is designed to support exchanging clinical and administrative data between systems.
Tie QA to observable outcomes: minimum dataset completeness, disposition correctness, routing accuracy, and confirmed handoff status, not subjective good calls.
Standardization is not only an efficiency play. It is also a control: it limits what gets collected, where it goes, and who can see it.
If you are handling protected health information, align intake capture and access controls to the HIPAA Privacy Rule, including the idea of limiting use and disclosure to what is needed for the task.
Operationally, this often means role-based access, clean audit trails, and secure handling expectations consistent with the HIPAA Security Rule.
When you use vendors to support intake or answering services, many organizations rely on contract terms and safeguards described in HHS guidance on business associate contracts to clarify responsibilities.

Deterministic routing and shared standards let overflow and after-hours coverage produce the same clean records as daytime intake.
Even if your intake team is not building integrations, interoperability expectations affect how you design your processes. The ONC information blocking program reflects a broader push toward timely access and exchange of electronic health information, which increases pressure to keep patient data structured, retrievable, and portable.
Legal intake is often time-sensitive, emotionally charged, and detail-heavy. Standardized capture reduces the chance that key facts are lost, but it also reduces unnecessary collection that can create risk in storage and access.
In practice, many firms implement structured must-have fields for conflicts and eligibility, then control narrative details in restricted notes with clear internal access rules.
Objective escalation triggers and urgency levels move time-sensitive contacts to the right path instead of waiting in a general queue.
If your organization is modernizing intake now, the bigger shift is that handoff quality is increasingly tied to interoperability and auditability requirements, not just internal efficiency.
ONC's HTI-1 final rule updated the health IT certification landscape, reinforcing expectations around standardized data and API-enabled exchange that can influence how EHR-adjacent workflows are designed.
CMS also expanded interoperability expectations through the CMS Interoperability and Prior Authorization final rule (CMS-0057-F) fact sheet, which is pushing more healthcare data exchange through standardized, API-oriented approaches over time.
Capture who, when, and how each entry was made. Provenance stamps let QA diagnose issues and support audit trails in regulated intake.
Quality monitoring works best when it measures observable behaviors and record outcomes, not subjective good calls. Tie QA to the minimum dataset, disposition correctness, and handoff status.
The sample checklist below can be adapted to legal, healthcare, and enterprise service intake.
Standardized, API-enabled exchange is becoming the expectation. Structured, portable data keeps you ready as interoperability rules expand.
Mistake 1: We just need more training. Training helps, but it cannot compensate for ambiguous fields, overlapping dispositions, or missing validation. Fix the system so correct capture is the path of least resistance.
Mistake 2: More fields means better intake. More fields often means more abandonment and more inaccuracies. Focus on the minimum viable dataset, then add expansion fields selectively using conditional logic and clear definitions.
Mistake 3: We can clean it up later with reports. Retrospective cleanup is expensive and never ends. Validation at capture and deterministic routing are cheaper than downstream remediation.
Mistake 4: Integration will solve it. Integration only moves data faster. If your definitions are inconsistent, integration accelerates inconsistency into every system.
Standardization succeeds when it is rolled out like an operational product: defined, piloted, measured, and governed. The list below is a proven sequence for high-volume inbound environments.
Define, pilot, measure, and govern. Sequence the rollout from minimum dataset and disposition dictionary to validation, handoff status, QA, and change governance.
If you are redesigning intake capture, dispositions, and CRM/EHR handoffs for scale, Go Answer can help you map the minimum dataset, standardize wrap-up codes, and implement QA so overflow and after-hours coverage stays consistent.
Request Pricing, Book a Discovery Call, or Talk to a Specialist to review your current intake workflow and identify the highest-impact standardization and handoff fixes.
If you are exploring options internally, you can also align stakeholders around these next steps: Explore Enterprise BPO, See How It Works, and View Use Cases.
Learn why thousands of companies rely on Go Answer.
Try us risk-free for 14 days!
Enjoy our risk-free trial for 14 days or 200 minutes, whichever comes first.
Have more questions? Call us at 888-462-6793
Learn why thousands of companies rely on Go Answer.
Have more questions? Call us at 888-462-6793
If you would like to get in contact with a Go Answer representative please give us a call, chat or email.

Thanks for your interest!
A representative will be reaching out to you shortly.
Have more questions? call us on 888-462-6793
